you may also like
Since the first FDA approval in 2017, CAR-T cell therapy has fundamentally reshaped the oncology treatment paradigm. However, the conventional "ex vivo" approach—which involves harvesting a patient's cells, modifying them in a lab, and reinfusing them—remains a severe logistical bottleneck. This "bespoke", slow and complex process takes 4-6 weeks and incurs prohibitive costs ranging from USD $450,000- $500,000 per treatment course, significantly limiting patient access.
To overcome these barriers to global scalability, the field is pivoting toward a groundbreaking solution: In Vivo CAR-T. By utilizing viral vectors or lipid nanoparticles (LNPs) to generate CAR-T cells directly inside the patient's body, this approach promises standardized manufacturing, "off-the-shelf" availability, and substantially reduced costs.
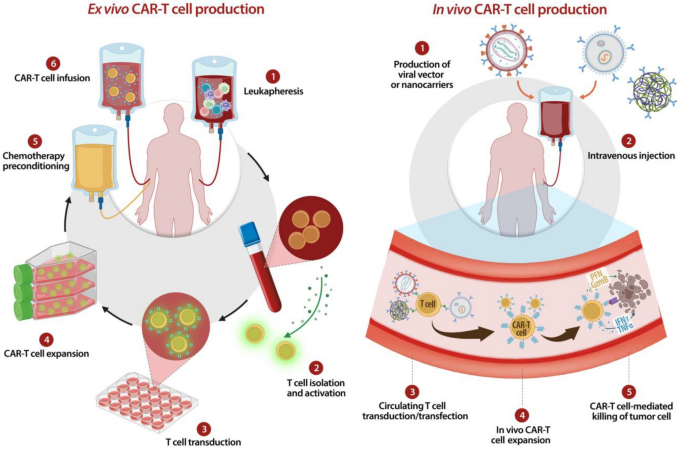
Ex vivo v.s. In vivo CAR-T cell production. (Pinto et al. 2025)
As we move through 2025 and 2026, the race to make in vivo CAR-T a clinical reality has intensified.
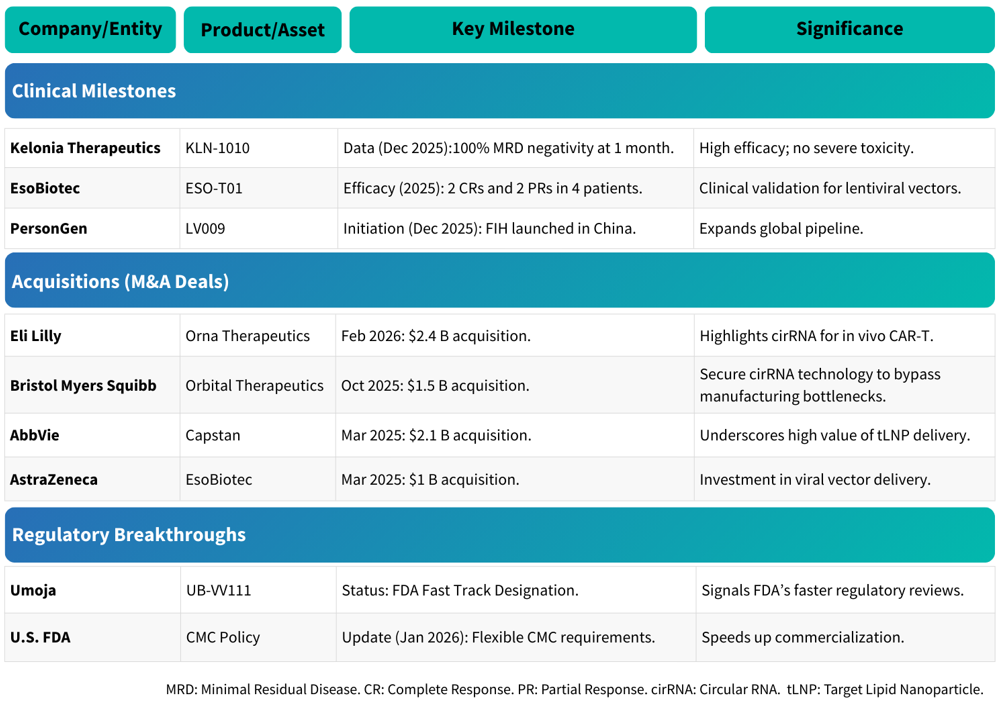
Recent Milestones in the In Vivo CAR-T Landscape (2025-2026).
Despite these rapid advances, in vivo CAR-T development faces significant hurdles. Because the host's body acts as the manufacturing plant, researchers must ensure precise delivery, avoid non-specific transduction, and finely control CAR expression levels.
This makes the choice of preclinical models critical. Researchers need models that can evaluate transduction efficiency (how well the vector hits the target) and functional immunity (how well the resulting CAR-T cells kill the tumor).
Leveraging advanced technology platforms, Biocytogen supports this critical transition by providing immunodeficient and humanized mouse models explicitly designed to de-risk in vivo CAR-T challenges
To extend the experimental window for testing viral vectors or bispecifics, Biocytogen engineered the B-NDG MHC I/II DKO mice plus.
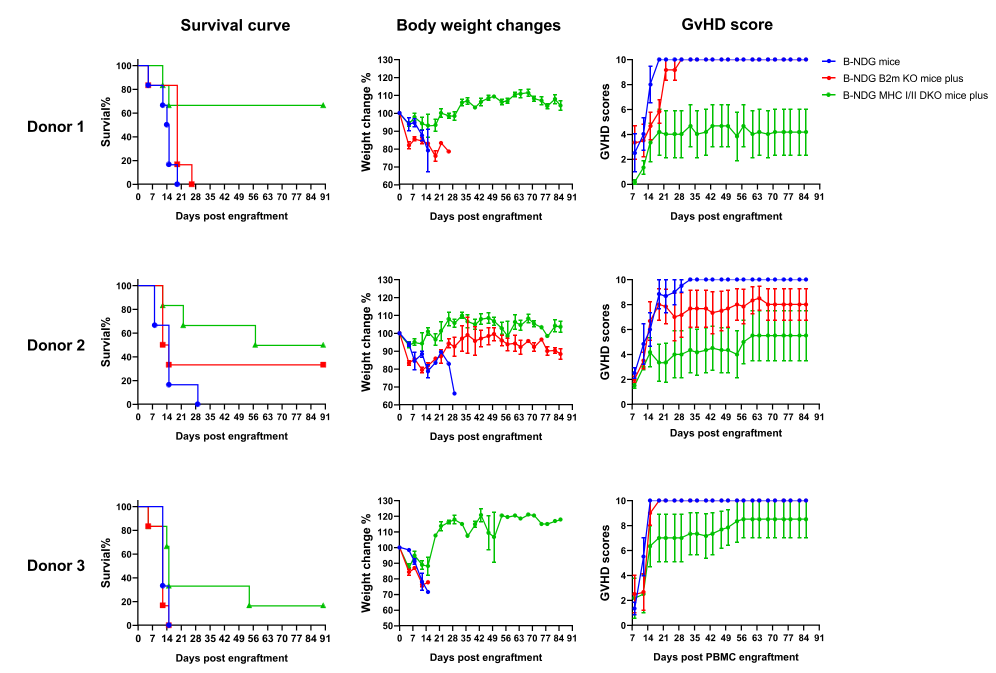
Figure 1. Reduced GvHD severity and extended survival in B-NDG MHC I/II DKO mice following human PBMC engraftment. Human PBMCs from three independent donors were engrafted into standard B-NDG (blue), B-NDG B2m KO plus (red), and B-NDG MHC I/II DKO plus (green) mice and monitored for survival, body weight changes and GvHD severity.
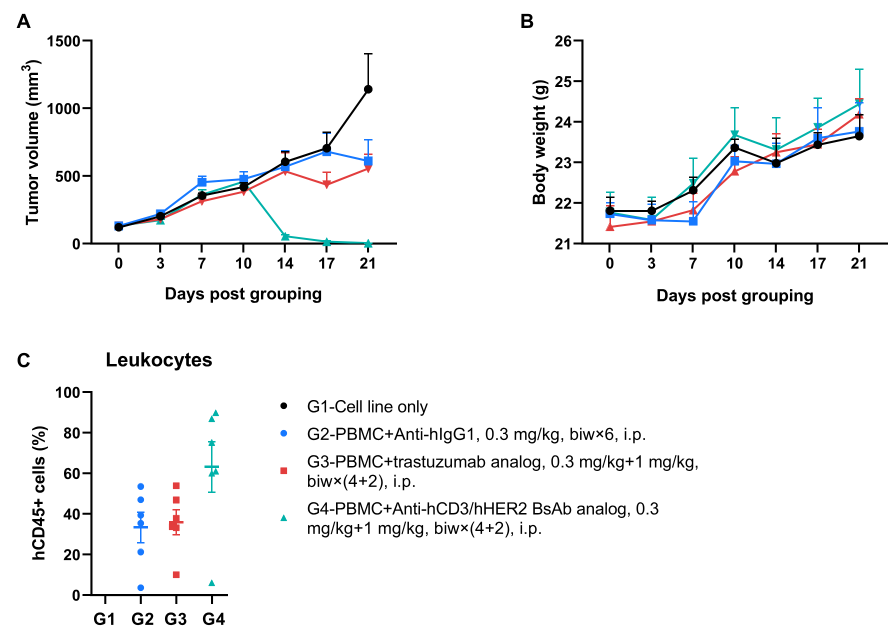
Figure 2. Robust tumor regression induced by anti-hCD3/hHER2 TCE in PBMC-engrafted B-NDG MHC I/II DKO Mice Plus. The human gastric cancer CDX model was established in B-NDG MHC I/II DKO mice plus via subcutaneous inoculation of HER2-positive NCI-N87 cells (1×10⁷), followed by intravenous engraftment of human PBMCs (1×10⁷). Control, anti-human CD3/HER2 TCE (in-house), and a benchmark trastuzumab analog (in-house) were administered intraperitoneally beginning 3 days after tumor inoculation. (A) Longitudinal tumor volume measurements revealed significant growth inhibition compared with the benchmark treatment. (B) Body weight tracking indicated no significant treatment-related toxicity. (C) Endpoint analysis of peripheral blood by flow cytometry. Data are presented as mean ± SEM.
For therapies that utilize viral vectors and LNPs to generate CAR-T cells directly within the body, the preclinical model must express the necessary human target to enable precise delivery and efficient CD8+ T-cell transduction.
The next 3-5 years represent a critical inflection period for in vivo CAR-T. As the industry pushes toward scalable solutions, the ability to generate reliable preclinical data will define success. Biocytogen’s robust portfolio provides the physiological relevance needed to translate innovative concepts into clinical reality. 👉 Contact us today to learn more!
In vivo CAR-T represents a transformative shift with both clinical and commercial benefits. Clinically, it streamlines treatment by eliminating complex ex vivo cell manufacturing, reducing vein-to-vein time and enabling faster patient access. Commercially, it supports scalable, standardized production with true off-the-shelf potential, significantly lowering manufacturing and supply chain costs. Together, these advantages improve accessibility and position the modality to expand beyond hematologic malignancies into solid tumors and potentially non-oncology indications.
While in vivo CAR-T offers disruptive advantages like "off-the-shelf" potential and lower costs, it faces significant preclinical hurdles. The core challenges include ensuring precise T-cell targeting, avoiding non-specific transduction (accidental modification of non-target cells), and maintaining fine control over CAR expression levels and duration to guarantee safety. Overcoming these requires rigorous testing in advanced mouse models to evaluate delivery strategies, expansion kinetics, and potential toxicity.
A major limitation in preclinical studies requiring human PBMC engraftment (like testing viral vectors) is the rapid onset of Graft-versus-Host Disease (GvHD), which severely limits the experimental window. Biocytogen's B-NDG MHC I/II DKO mice plus solve this by knocking out MHC class I and II molecules, significantly delaying GvHD. Post-transplantation survival in these mice can exceed 100 days, and they maintain human T cell proportions near 100% for up to 16 weeks, allowing for extended, reliable efficacy tracking.
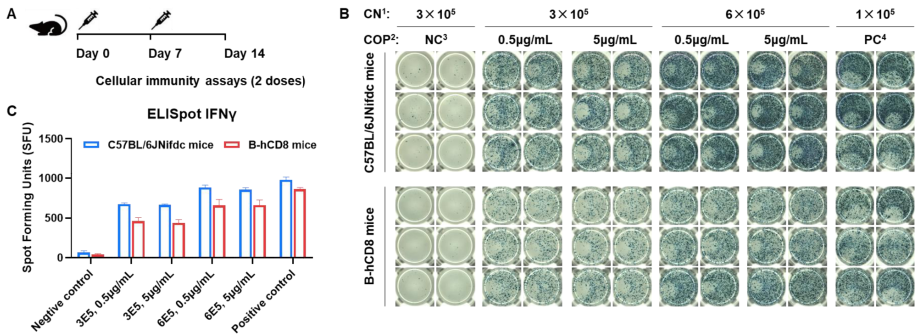
In vivo CAR-T approaches targeting human CD8⁺ T cells require a host that expresses human CD8—ensuring precise viral entry and efficient CD8+ T-cell transduction. Biocytogen's B-hCD8 mice express human CD8 and are proven to possess normal T cell immune function—under OVA stimulation, these mice can normally secrete IFN-γ at levels comparable to wild-type controls. This ensures that any anti-tumor efficacy observed in your study is a true reflection of your therapeutic design.