In vivo T-cell engagers (TCEs) are rapidly becoming a central trend in immuno-oncology. While first-generation TCEs validated the power of redirecting endogenous T cells to tumors, their short half-life, continuous infusion requirements, and manufacturing complexity have limited broader development. As the field seeks more durable, controllable, and scalable immune activation strategies, attention has shifted toward platforms that enable sustained TCE expression directly within the patient.
mRNA-encoded T-cell engagers (mRNA-TCEs) represent one of the most promising advancements in this space. By combining the clinically validated biology of bispecific T-cell redirection with the flexibility and tunability of mRNA delivery, mRNA-TCEs offer programmable in vivo production, improved pharmacokinetic control, and a streamlined path toward scalable next-generation immunotherapy.
► Why mRNA-Encoded T Cell Engagers?
Challenges of Protein-Based T-Cell Engagers
Bispecific TCEs work by acting as molecular bridges, simultaneously grabbing a tumor-associated antigen (TAA) and the CD3 receptor on a T cell. This forced "handshake" activates the T cell to kill the tumor, regardless of its original target.
While protein-based TCEs have shown success in hematologic cancers (leukemia and lymphoma), solid tumors remain challenging due to:
- Poor Penetration: Large proteins struggle to penetrate dense tumor tissues.
- Systemic Toxicity: Short half-lives often require continuous infusion, leading to “peak-and-trough” dosing that increases the risk of cytokine release syndrome (CRS).
- Manufacturing Complexity: Recombinant proteins are expensive, slow to produce and technically demanding to scale.
Advantages of mRNA-Encoded T Cell Engagers
In vivo mRNA delivery addresses these challenges. Instead of injecting the protein, administration of mRNA leverages endogenous protein synthesis—it instructs the patient's own cells to produce the TCEs. This allows for:
- Transient & Controllable Expression: More precise control over how much and for how long the drug is active.
- Superior Bioavailability: Localized, continuous production maintains a steady therapeutic window, improving tumor penetration and distribution within the immunosuppressive tumor microenvironment (TME).
- Reduced Immunogenicity: mRNA delivery minimizes neutralizing anti-drug antibody formation compared to recombinant proteins.
► Recent Breakthrough: From Proof-of-Concept to the Clinic
Preclinical and Clinical Momentum in In Vivo mRNA-TCEs:
- Foundational proof-of-concept: In 2017, Stadler et al. Nat. Med. showed that mRNA-encoded bispecific antibodies could drive effective T-cell-mediated tumor suppression in vivo, establishing a scientific basis for the approach.
- Modularity and immune enhancement: In 2024, Hangiu et al. Front. Immunol. described an mRNA-encoded bispecific system that combines T-cell engagement with PD-L1-dependent 4-1BB co-stimulation, enhancing antitumor activity while potentially broadening the therapeutic window.
- Moderna's multi-target strategy: Moderna’s mRNA-2808 encodes three TCEs targeting validated myeloma antigens to address heterogeneity and resistance mechanisms (Garnaas et al. 2024). In 2025, the first patient was dosed in a Phase 1/2 trial in relapsed or refractory multiple myeloma (RRMM), marking the company’s first-in-human mRNA-TCE study and a key clinical milestone (Press Release).
- METiS TechBio's targeted delivery advances: In 2025, Huang et al. Nat. Commun. demonstrated organ-specific delivery of MTS-105, a glypican-3-targeted mRNA-TCE, with improved local efficacy and reduced systemic toxicity in hepatocellular carcinoma models, highlighting the potential of organ-selective mRNA delivery to expand the therapeutic window in solid tumors.
► Accelerating mRNA-TCE Translation: Biocytogen's Solution
Target Humanized Mouse Models:
As mRNA-TCEs transition from concept to clinic, the ability to model their activity in physiologically relevant systems is critical. Because TCEs rely on high-affinity binding to human CD3, standard mouse models are often insufficient for efficacy or safety testing.
Biocytogen’s target humanized TCE mouse models provide the essential validation platform needed for IND-enabling studies. By replacing one or multiple mouse targets with their human counterparts (e.g., human CD3, PD-1, or TAAs), these models allow researchers to evaluate:
- Human-Relevant Efficacy: Measure T-cell-mediated tumor lysis in a physiologically relevant system.
- Safety & Cytokine Profiles: Predict potential cytokine release syndrome (CRS) and on-target/off-tumor toxicities.
- PK/PD Optimization: Track the expression kinetics of the mRNA-encoded protein to optimize dosing schedules.
See Case Study #1 for how we evaluate TCE efficacy in our mouse model!
Immunodeficient Mouse Models:
Case Study #2 is a perfect example of how Biocytogen’s advanced immunodeficient mouse models, such as B-NDG MHC I/II DKO mice plus, address key challenges in mRNA-TCE development:
- Extended Study Window: By knocking out mouse β2-microglobulin and MHC I/II—the "ID tags" T cells use to identify foreign components—Biocytogen significantly delays human T-cell-mediated graft-versus-host disease (GvHD). This extends the evaluable study window, enabling robust assessment of long-term mRNA-TCE efficacy and safety without premature mouse mortality.
- Human-Relevant Context: Through PBMC engraftment, researchers can evaluate how mRNA-TCEs activate actual human T cells against a human tumor antigen (e.g., HER2) in vivo.
- High-Fidelity Efficacy & Safety Data: The ability to track both tumor volume and human leukocyte expansion allows accurate mapping of the therapeutic index of the candidate.
 Case Study 1: Efficacy of CD3/CD20-Targeting TCE in B-hCD3EDG/hCD20 Model
Case Study 1: Efficacy of CD3/CD20-Targeting TCE in B-hCD3EDG/hCD20 Model
Antitumor Efficacy of Glofitamab (a CD3/CD20-Targeting TCE):
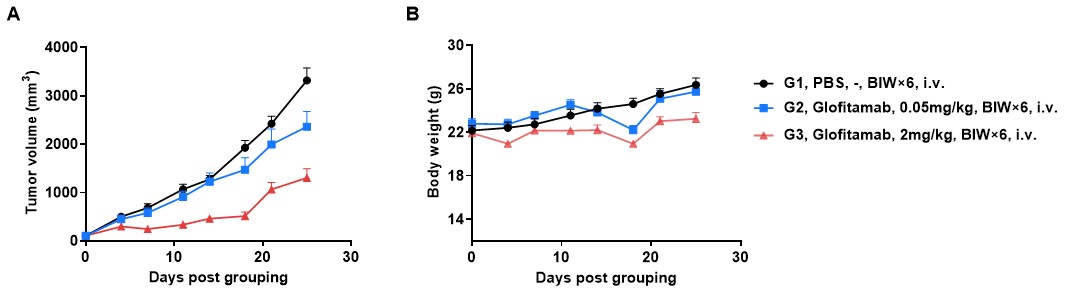
B-hCD20 MC38 colon carcinoma tumors were established subcutaneously in B-hCD3EDG/hCD20 mice, which then received intravenous administration of Glofitamab, an anti-human CD3/CD20 bispecific T-cell engaging antibody. (A) Glofitamab inhibited tumor growth in a dose-dependent manner in B-hCD3EDG/hCD20 mice bearing B-hCD20 MC38 tumors. (B) Body weights remained stable throughout the treatment. Data are presented as mean ± SEM.
Glofitamab Demonstrated Dose-Dependent B-Cell Depletion:
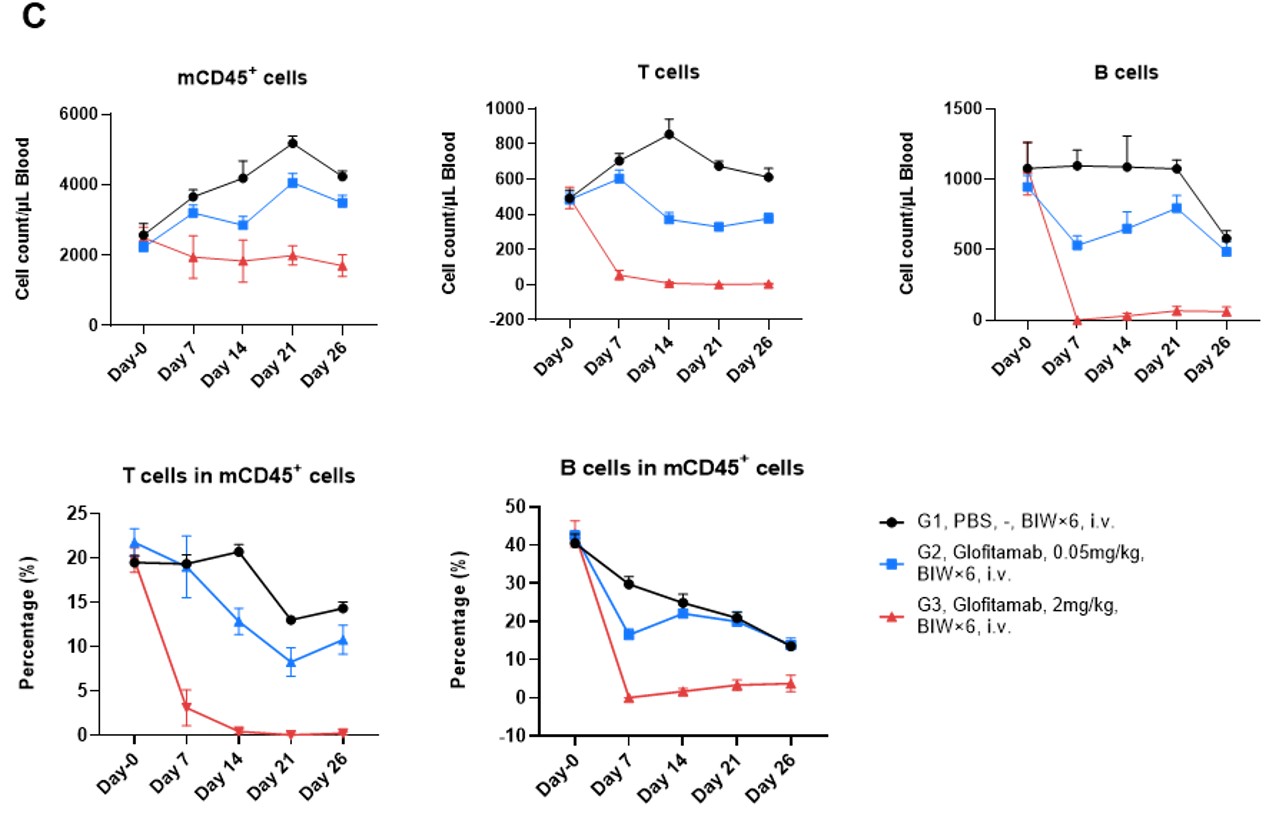
Peripheral blood was collected on indicated timepoints. Absolute cell counts and frequencies of leukocytes (mCD45⁺), B cells (mCD19⁺), and T cells (mTCRβ⁺) were quantified by flow cytometry. Glofitamab induced sustained and dose-dependent depletion of B cells—consistent with antitumor efficacy of CD20 antibody, and T-cell loss. Data are presented as mean ± SEM.
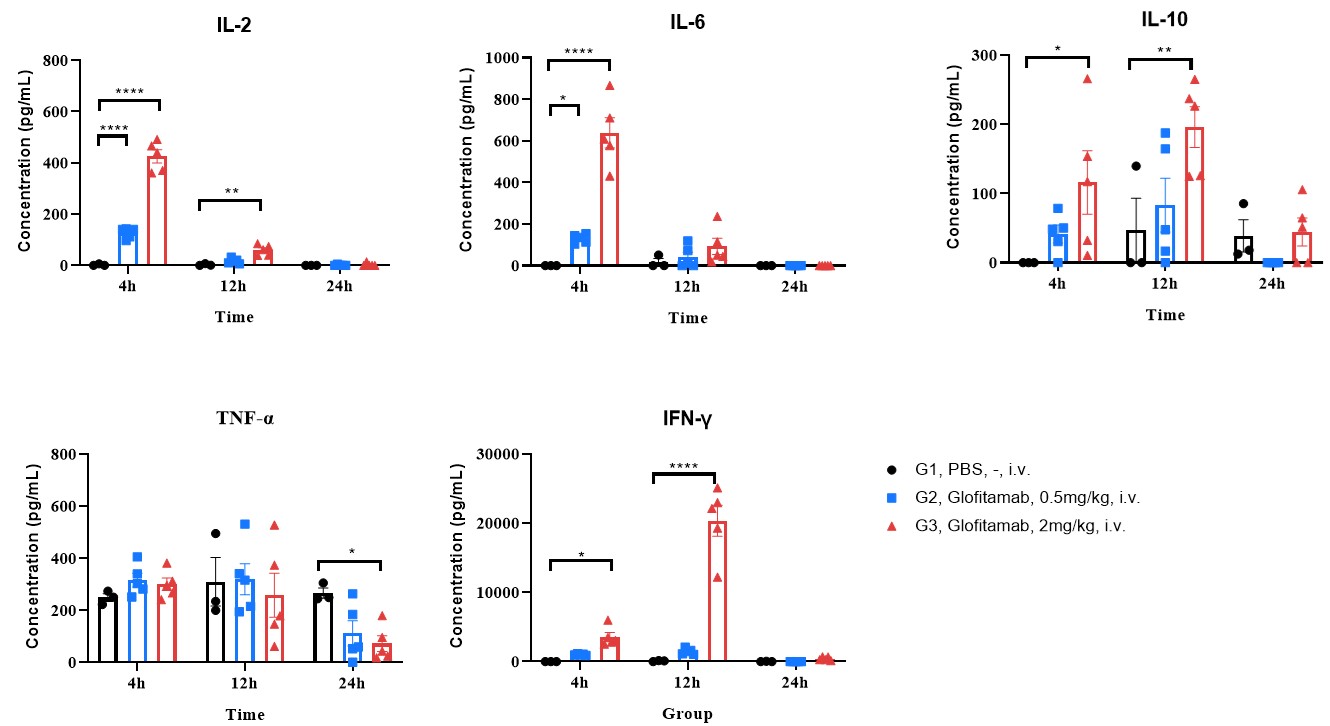
Glofitamab Triggered Cytokine Release:
Blood was collected and analyzed for cytokine concentration at indicated timepoints after the first dosing. Glofitamab induced dose-dependent increases of multiple cytokines within the first 12 hrs after dosing. Data are presented as mean ± SEM. Significance was determined by two-way ANOVA test. *P<0.05, **P<0.01, ****P<0.001.
Case Study 2: Efficacy of CD3/HER2-Targeting TCE in a Gastric Cancer CDX Model
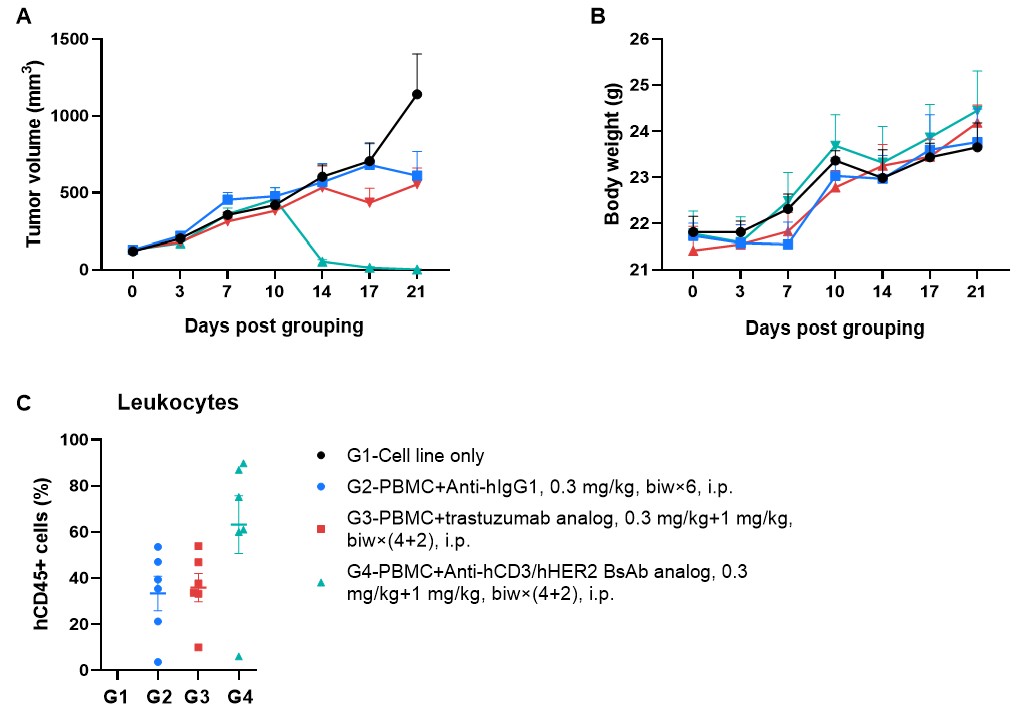
Robust Tumor Regression Induced by Anti-hCD3/hHER2 TCE in PBMC-Engrafted B-NDG MHC I/II DKO Mice Plus. The human gastric cancer CDX model was established in B-NDG MHC I/II DKO mice plus via subcutaneous inoculation of HER2-positive NCI-N87 cells (1×10⁷), followed by intravenous engraftment of human PBMCs (1×10⁷). Control, anti-human CD3/HER2 TCE (in-house), and a benchmark trastuzumab analog (in-house) were administered intraperitoneally beginning 3 days after tumor inoculation. (A) Longitudinal tumor volume measurements revealed significant growth inhibition compared with the benchmark treatment. (B) Body weight tracking indicated no significant treatment-related toxicity. (C) Endpoint analysis of peripheral blood by flow cytometry. Data are presented as mean ± SEM.
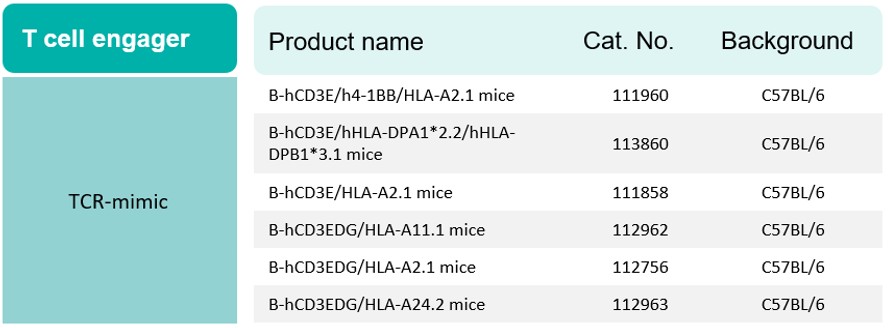
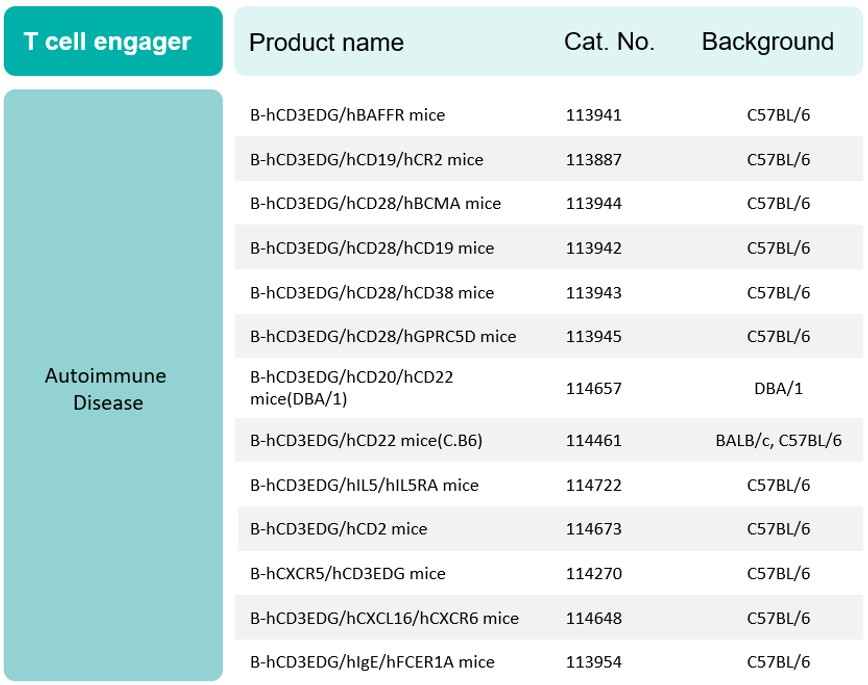
► Biocytogen's Extensive Portfolio Supporting Next-Gen TCE Research:
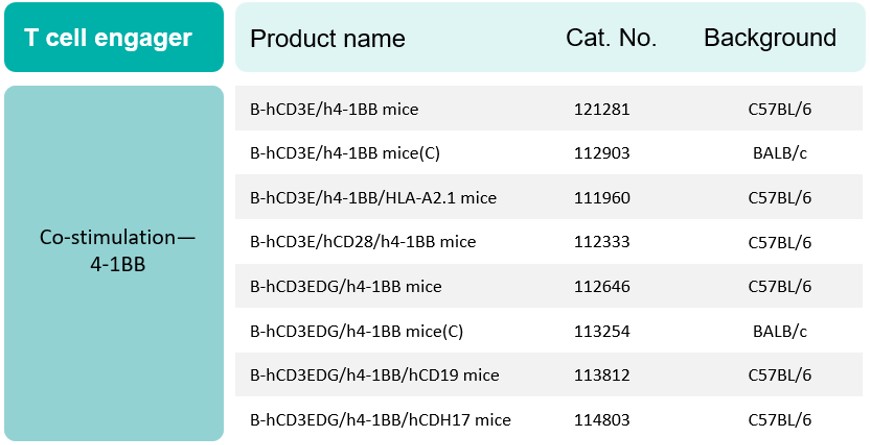
To support diverse therapeutic pipelines, Biocytogen offers an extensive portfolio of high-demand, target-humanized mouse models—including CD3, 4-1BB, and dual-target or multi-target strains—specifically validated for next-generation TCE research.
- Comprehensive Humanization: Humanized for CD3E, CD3D, and CD3G, the CD3EDG humanized mouse model enables accurate evaluation of human CD3-targeting TCEs, validated through both in vitro T-cell activation and in vivo efficacy assays.
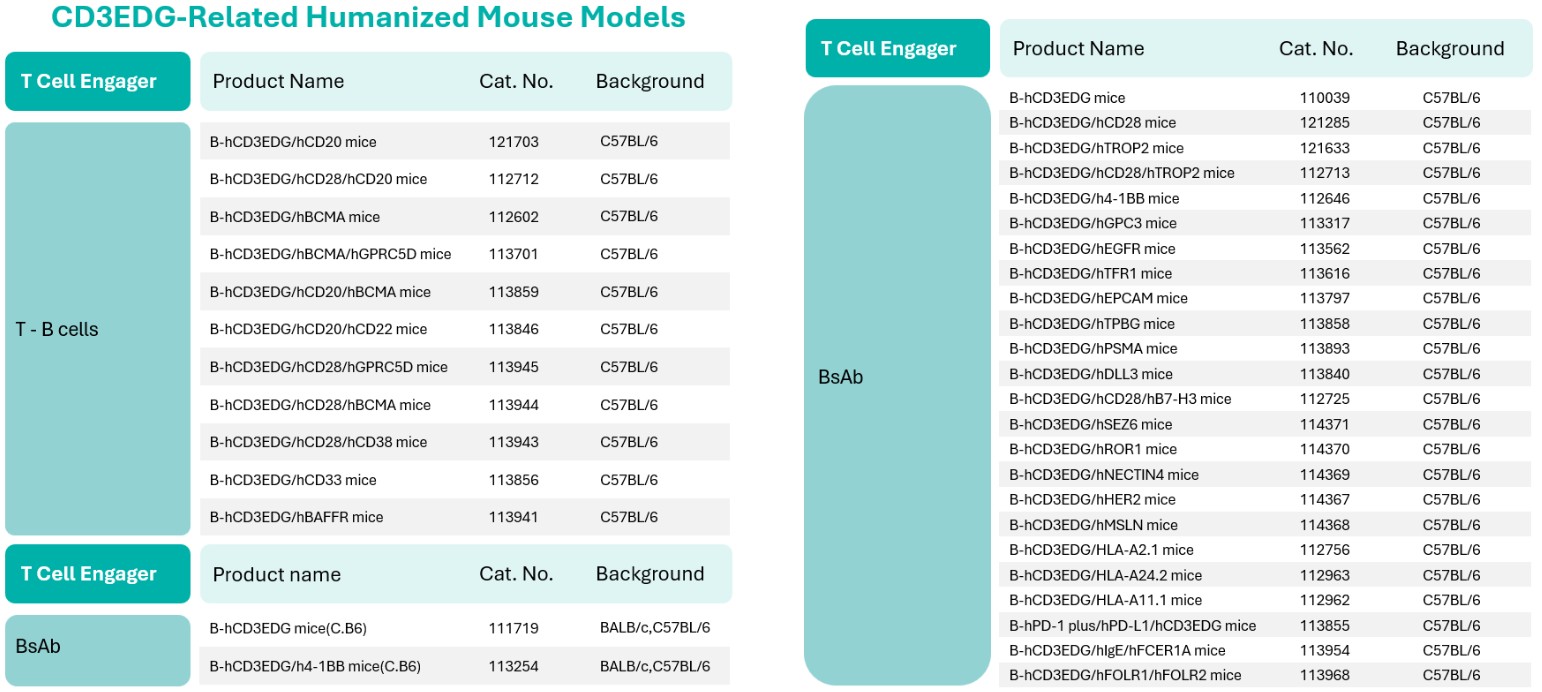
- Enhanced Anti-Tumor Activity: Engagement of the 4-1BB co-stimulatory molecule enhances T-cell proliferation and sustains long-term antitumor responses. The humanized 4-1BB knock-in model enables accurate evaluation of this co-stimulatory mechanism in a physiologically relevant setting.
- HLA-Restricted TCR-Mimic Support: Specialized B-hCD3EDG models provide a human-relevant platform to assess TCR-mimic TCEs with high confidence.
- Autoimmune Disease Applications: A dedicated suite of B-hCD3EDG models supports the translational development of TCEs for autoimmune disease indications (partial list).
👉 Contact us today for data packages or the full catalog of our B-hCD3EDG double-humanized models for specific tumor antigens!
Frequently Asked Questions (FAQs)
1. Why are humanized mouse models essential for mRNA-TCE research?
Traditional mice cannot evaluate TCEs because these therapies are designed to bind specifically to "human" CD3 and tumor-associated antigens (TAAs). Biocytogen’s target humanized mice, such as the B-hCD3 series, provide the necessary human receptors to validate in vivo efficacy, T-cell recruitment, and tumor-killing mechanics in a physiologically accurate system.
2. How does mRNA delivery compare to recombinant proteins in these models?
mRNA delivery leverages endogenous protein synthesis, which minimizes neutralizing anti-drug antibody (ADA) formation compared to traditional recombinant proteins. Our models allow for head-to-head comparisons to optimize tissue distribution, programmable expression, and repeat-dosing schedules.
3. How do B-NDG MHC I/II DKO mice plus improve the testing window for mRNA therapies?
Knockout of β2-microglobulin (B2m) and MHC I and II molecules renders the mouse functionally “invisible” to engrafted human T cells, significantly delaying graft-versus-host disease (GvHD). This extends the experimental window, allowing researchers to evaluate long-term efficacy and PK/PD correlations without interference from premature mouse mortality due to GvHD.
4. What translational endpoints can be measured in these models?
Biocytogen’s platforms enable high-fidelity tracking of key clinical indicators:
- Human Target Engagement: Confirmation of T-cell/tumor cell interaction and activation.
- PK/PD Optimization: Monitoring the kinetics of mRNA-encoded protein production in blood.
- Immune Phenotyping: Tracking the expansion of human leukocytes and T-cell activation markers.
- Efficacy & Safety Profiling: In vivo evaluation of tumor response, cytokine release patterns, and treatment-related tolerability to support therapeutic window assessment.